CORRECT ANSWER IS C
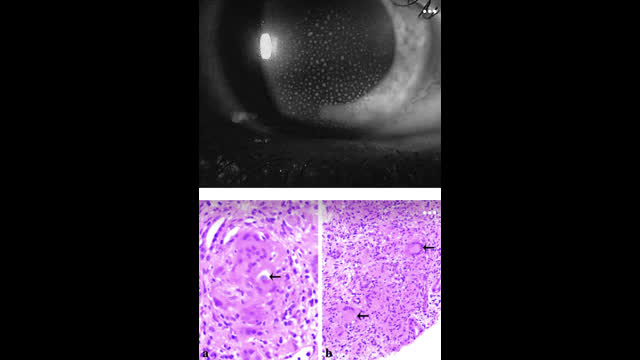
Patient has features of anterior uveitis on slit exam exam (corneal precipitates) and renal biopsy shows evidence of Granulomatous interstitial nephritis (GIN) with non-caseating granulomas with foreign body-type giant cells. (See arrows). Lupus is not associated with Granulomatous interstitial nephritis (GIN). Immunofluorescence did not reveal full house pattern of Immunoglobulin deposition. Lupus patients usually have low C3 and C4 levels during disease flares because of activation of the complement system by immune complexes. This patient had only low c3 levels in serum.
GIN is a rare entity detected in ∼0.5–0.9% of all renal biopsies. GIN has been linked to several antibiotics such as cephalosporins, vancomycin, nitrofurantoin and ciprofloxacin, non-antibiotic drugs such as Dilantin, allopurinol, Omeprazole, Heroin, alendronate etc. It is also associated with NSAIDs and infections such as tuberculosis, fungal infections and after Intestinal bypass, Oxalosis. Inflammatory/rheumatology conditions such as granulomatosis with polyangiitis, Sarcoidosis, TINU syndrome, Crohn’s disease, Granulomatosis with polyangiitis (GPA), Eosinophilic granulomatosis with polyangiitis (EGPA), Bacillus Calmette–Guerin therapy are other associated conditions.
TINU syndrome –
TINU syndrome is defined by the combination of tubulointerstitial nephritis and uveitis. Most patients with TINU are adolescents and young women. Renal manifestations include flank pain, sterile pyuria, hematuria, proteinuria (usually sub nephrotic range), kidney function impairment, and acute kidney injury (AKI). Proximal and distal tubular defects can be seen, resulting in phosphaturia, and acidification defects, aminoaciduria, glucosuria. uveitis usually present with bilateral eye pain or redness. While granulomas on renal biopsy are less common in TINU, they are the defining lesion in renal sarcoidosis.
Primary Sjögren’s syndrome (pSS) is an autoimmune disease characterized by lymphocytic and plasmocytic infiltration of the exocrine glands. It can present with anterior and posterior uveitis. Tubulointerstitial nephritis (TIN) is the most common type of renal involvement in pSS. Granulomatous interstitial nephritis (GIN) with presence of granulomas against a background of interstitial inflammation is not a typical and commonly seen form of TIN in pSS but has been described in case reports.
Sarcoidosis –
Sarcoidosis is a systemic disease characterized by chronic non‐caseating granulomatous inflammation with tissue destruction. Most common clinical features being bilateral hilar lymphadenopathy, skin lesions and pulmonary infiltrates. Uveitis is a frequent (20-50%) and early feature of sarcoidosis. Typical sarcoid uveitis presents with mutton-fat keratic precipitates on cornea, iris nodules, and anterior and posterior synechiae. Posterior involvement includes vitreitis, vasculitis, and choroidal lesions. The most common cause for renal failure in sarcoid is hypercalcemia leading to nephrocalcinosis, nephrolithiasis or reversible dysfunction due to hypovolemia. Renal failure in sarcoidosis can also be caused by granulomatous interstitial nephritis (GIN), which is reportedly present in approximately one‐third of patients with clinical evidence of renal disease and sarcoid. This patient has hypercalcemia and uveitis, and sarcoidosis work up needs to performed.
Reference
Sarcoidosis and uveitis – PubMed (nih.gov)
Renal Disease in Primary Sjögren’s Syndrome – PubMed (nih.gov)
Granulomatous interstitial nephritis associated with Primary Sjögren’s syndrome – PubMed (nih.gov)
