Correct Answer is (B)
Pembrolizumab is an immune-checkpoint inhibitor (ICI), designed as a highly selective anti-programmed death-1 (PD-1) humanized monoclonal antibody. It inhibits the negative immune regulation due to PD-1 receptor signaling enabling anti-tumor response and reverses T cell suppression. It has been approved for numerous malignancies, including gastric, ovarian, non-small cell lung cancer, and melanoma.
Cortisol deficiency impairs renal excretion of free water and increases the plasma level of antidiuretic hormone, vasopressin (AVP), reduces the expression of vasopressin 2 receptors (V2R), decrease aquaporin expression resulting in dilutional hyponatremia.
Primary adrenal insufficiency is caused by adrenocortical failure and is manifested by low aldosterone level, high ACTH level,and elevated renin levels. While adrenal metastasis is possible in malignant melanoma, normal aldosterone levels make it less likely to be the case.
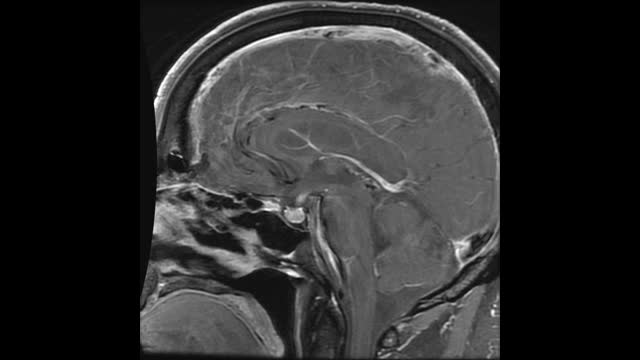
Secondary adrenal insufficiency develops from impairment of the pituitary gland. Pembrolizumab can cause hypophysitis in a small percentage of patients (< 1%) resulting in low ACTH secretion and secondary adrenal insufficiency. Patient likely developed secondary adrenal insufficiency given his inappropriately low normal ACTH level in setting of symptoms of adrenal insufficiency. Subnormal response to ACTH stimulation test is confirmatory for adrenal insufficiency.
Hypothyroidism is not direct causation of hyponatremia. Hypothyroidism decreases cardiac output and subsequently increases plasma antidiuretic hormone (ADH) concentration and water retention resulting in hyponatremia. Hyponatremia is usually seen in patients with severe hypothyroidism leading to myxedema coma and reduced cardiac output. He has no clinical evidence of myxedema coma or low cardiac output.
Cerebral salt wasting (CSW) is another potential cause of hyponatremia in those with CNS disease, particularly patients with tumors or subarachnoid hemorrhage. CSW is characterized by hyponatremia and extracellular fluid depletion (hypovolemia) due to inappropriate sodium wasting in the urine. Two common proposed mechanisms for this include release of brain natriuretic peptide (BNP) after CNS injury, entering systemic circulation through a disrupted blood-brain barrier. The BNP acts on the collecting ducts of the renal tubules to inhibit sodium reabsorption as well as decrease the release of renin. The other proposed mechanism is injury to sympathetic nervous system causing a failure of renin release and sodium reabsorption. The exact mechanism of cerebral salt wasting remains unclear. Patient does not have any signs of ECF depletion. (Normal hematocrit, BP, moist mucous membranes)
Reference
Hyponatraemia secondary to nivolumab-induced primary adrenal failure – PMC (nih.gov)
