A. Patient most likely has amphotericin B induced nephrotoxicity due to use of Non liposomal preparation. Amphotericin can cause acute kidney injury both due to direct toxic effect on renal tubules and also also from renal vasoconstriction due to direct effect of amphotericin B on renal vasculature and from acute tubular glomerular feedback mediated by increased sodium entry into juxtaglomerular cells mediated by increased ion permeability induced by enhanced membrane permeability due to Amphotericin.
Amphotericin also causes increased urinary potassium wasting, hypokalemia, increased urinary magnesium wasting and low serum magnesium levels, type 1, distal RTA. It also causes polyuria due to to nephrogenic diabetes by increasing resistance to ADH hormone. Hypokalemia induced by amphotericin can also cause nephrogenic diabetes insipidus by causing ADH hormone resistance
B. Osmolar diuresis from high BUN is associated with increased urine osmolality. However patient urine osmolality is low in the 100 mOsm/L range and does not explain polyuria. He also has acute kidney injury decreasing glomerular filtration making it less likely to have polyuria.
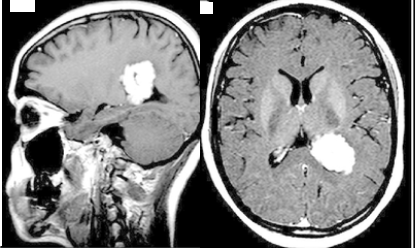
C. Metastatic CNS-posterior pituitary lesions from myeloma can cause central diabetes insipidus. MRI of the brain revealed a lobulated mass in left lateral ventricle trigone Which is not associated with ADH deficiency. Lack of response to desmopressin challenge also makes central diabetes insipidus less likely.
D. Patient’s hypercalcemia is very mild and does not explain this to polyuria. Hypercalcemia can cause decreased sodium chloride reabsorption in the ascending limb of the renal tubules decrease in medullary osmotic gradient making ADH hormone ineffective.
References
- [Nephrogenous diabetes insipidus caused by amphotericin B] – PubMed (nih.gov)
- Amphotericin B-induced Nephrogenic Diabetes Insipidus in a Case of Cryptococcemia – Amphotericin B-induced nephrogenic diabetes insipidus in a case of cryptococcemia – PubMed (nih.gov)
